 by
Mamisoa Andriantafika
by
Mamisoa Andriantafika
Some days your vision is sharp; on others it blurs and fluctuates from one moment to the next. We readily blame fatigue, age or screens. Yet the first culprit is often invisible: the tear film that coats your eyes.
This film of tears, only a few microns thick, is far more than mere protection. It is the eye's first lens: its quality determines the sharpness of your vision, the reliability of your correction in glasses or contact lenses, and even the accuracy of the measurements taken before laser refractive surgery.
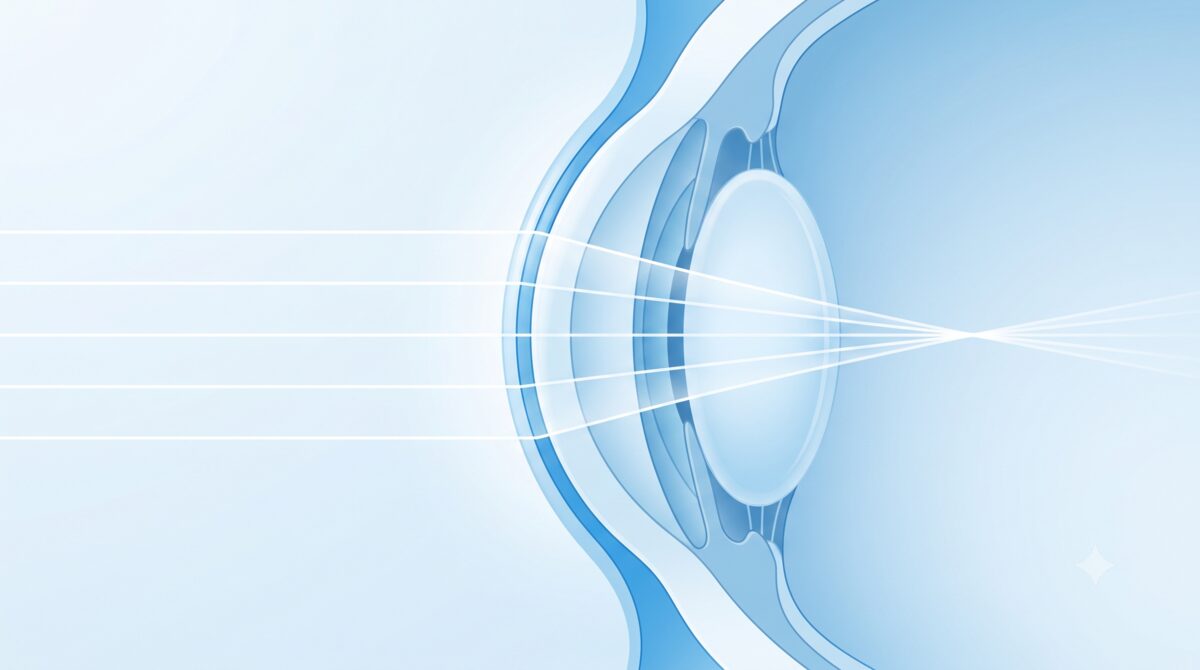
When we think about vision, we picture the cornea and the lens. Yet the very first surface that light meets as it enters the eye is not the cornea: it is the tear film resting on it. It is at this interface between air and tears that the largest jump in refractive index occurs, and therefore most of the eye's optical power.
In other words, a perfect cornea covered by an irregular tear film sees poorly. If the surface of the tears is bumpy, dry in places or unstable, light is scattered instead of being focused sharply on the retina.
The eye's first lens is not the cornea, but the tear film that covers it.
This film is a fragile balance of three components: a superficial lipid layer, produced by the meibomian glands, which prevents evaporation; an aqueous layer from the lacrimal gland; and a mucin layer that allows the tears to adhere to the cornea. The slightest defect in any one of them destabilises the whole.
The fact that vision changes with each blink is not always normal.
A stable tear film stays smooth for several seconds between two blinks. When it is of poor quality, it breaks up too quickly: the optical surface degrades within a few seconds and vision blurs, then clears as soon as you blink to reform the film. It is this instability that explains vision fluctuating over the course of the day.
Many patients describe vision that "comes and goes", blurrier at the end of the day, during prolonged reading or in front of a screen. It is not necessarily the eye tiring: it is often the tear film that no longer holds.
Screen work is a major factor, but not for the reason people think. The screen's "light" is often blamed, whereas the real problem lies elsewhere: the close working distance increases the effort of accommodation, and above all concentration sharply reduces the blink rate. The less you blink, the less the film is renewed, and the more it dries out. Air conditioning, heating and contact lens wear make the phenomenon worse still.

Here is one of the most common paradoxes in the consulting room: patients come in for watery eyes… and leave with a diagnosis of dry eye. "My eyes can't be dry, they water all the time," we often hear. Yet this is a misconception.
Two types of tears must be distinguished. Basal tears, permanent and of good quality, lubricate the eye continuously. Reflex tears, by contrast, are produced as an emergency response by the lacrimal gland when the surface of the eye is irritated — exactly as when you peel an onion.
Paradoxically, watering can be the first sign of a dry eye.

When the lipid layer is deficient (meibomian gland dysfunction), the film evaporates too quickly, and the cornea dries out and becomes irritated. The eye then reacts with a burst of reflex tears — abundant but watery and unstable — that overflow without ever correcting the underlying problem. Watering is therefore not the opposite of dryness: it is often its signal.
On an unstable surface, no measurement of eyesight is perfectly reliable.
Since the tear film is the eye's first lens, an unstable surface distorts the measurement of your correction. During a refraction, visual acuity changes from one moment to the next: the patient hesitates — "that's better… no, worse" — and the result varies between the start and the end of the examination. There is then a risk of an over- or under-corrected glasses prescription, lenses that are "never quite right" and contact lens intolerance.
Instrumental measurements are just as sensitive. Keratometry, corneal topography and aberrometry in fact analyse the surface of the tear film. On a dry eye, they return noisy, irregular maps that are hard to reproduce from one measurement to the next.
This is why it is essential to optimise the ocular surface first before finalising a precise correction. A healthy surface means a stable measurement — and therefore glasses or contact lenses that are genuinely suited to you.

What is true for a pair of glasses becomes critical before laser refractive surgery such as LASIK or PRK. Preoperative measurements — topography, aberrometry, biometry — are used to calculate the laser treatment to within a micron. Carried out on a dry surface, they are distorted from the outset.
A topography disrupted by an unstable film can simulate a corneal irregularity, lead to a miscalculation of the treatment, or even wrongly rule out a good candidate — or, conversely, mask a genuine contraindication. The reliability of the procedure depends directly on the quality of the surface at the time of measurement.
Before the laser, we never measure or operate on a dry surface.
There is also a key point to add: refractive surgery temporarily worsens dryness by severing some of the corneal nerves. An eye that is already dry before the operation will be more so afterwards. This is why uncontrolled dryness constitutes a contraindication, at least temporarily: we treat it first, then operate.
Optimising the ocular surface stabilises both the vision and its measurement.
The first step is an assessment of the ocular surface. We measure the tear film break-up time (BUT), examine the eyelid margins and the meibomian glands (meibography), and can evaluate the osmolarity of the tears. This assessment makes it possible to distinguish dryness caused by a lack of water from dryness caused by evaporation, which is the more common.
Management is progressive: treating the cause or the aggravating factor, adding suitable artificial tears, carrying out eyelid care (warming then massage to unclog the glands) and, if needed, supplementing with fatty acids. In meibomian gland dysfunction, treatment with IPL/LLLT pulsed light often makes it possible to restore a quality tear film over the long term.
The principle is always the same: optimise the surface before measuring or operating. It is the condition for stable vision, an accurate correction and successful refractive surgery.

Do not underestimate your tears. Vision that fluctuates, eyes that sting or water, a correction that is hard to stabilise: these subtle signals deserve an assessment of the ocular surface, especially if you are considering refractive surgery. A healthy tear film is the foundation of sharp vision and a reliable correction.
